Targeting Addiction
One man’s quest on the path of discovery
Tom remembers perfectly one intense sensation from the day he started his journey into alcoholism. The aroma of bourbon.
Even now, decades later, the seductive scent of sour mash whiskey lingers in his memory. So does the moment his life changed. He was watching his 12-year-old son play football. The game is forgotten, but Tom still recalls clearly just one man—an acquaintance who was a heavy drinker.
“He was constantly mixing and downing bourbon and Coke during the game,” Tom says. “I didn’t keep any hard liquor and didn’t drink much of it. But I caught a whiff and thought: ‘Man, that smells good.’ Shortly after that, I got a bottle, too, and that led me into drinking.”
Thousands of cocktails later—long after he switched from bourbon with its telltale odor to vodka’s bland anonymity—Tom realized that alcohol controlled his life. He planned his day around it, yearned for the first sip, got nervous if it was delayed and led an 80-proof social life. Tom knew that he was an alcoholic. That epiphany led him into the world of addiction research overseen by Dr. Bankole Johnson, chairman of the Department of Psychiatry and Neurobehavioral Sciences at the University of Virginia Medical School.
For 10 years, Johnson has intensely studied addictions and treatments for them. One overriding idea drives his work.
“My main goal is to find the right drug to treat the right person to get rid of addiction,” he says, while acknowledging that the complexities of the disease extend beyond a solely pharmaceutical approach.
Besides this, Johnson’s research has two other broad objectives. First, he wants to develop a computer model of the brain, which could aid design of new anti-addiction pharmaceuticals. Second, he wants to precisely define addiction, its functions and its effect on the brain. These aren’t fully grasped today. However, incremental progress is being made, aided by scientific breakthroughs and cutting-edge technologies, like brain imaging. Ultimately, doctors hope to comprehend the entire condition of addiction by first understanding its parts.
Johnson’s work has sparked international interest and intense media coverage. That’s no surprise. Drug and alcohol addiction is a disease affecting millions around the globe.
The world seems especially fascinated by Johnson’s study of topiramate, a pharmaceutical. HBO featured his research in Addiction, a documentary that received a 2007 Emmy award. Topiramate holds promise for modifying addictive behavior, especially alcoholism. Tests overseen by Johnson also are exploring its effect on cocaine and methamphetamine users.
While some specialists question the use of pharmaceuticals to treat addiction, Johnson’s work has won high praise. Medical experts describe it as a singular breakthrough in addiction treatment that advances scientific understanding of the disease to a new level. Dr. Pedro Ruiz, a professor in the Department of Psychiatry and Behavioral Sciences at the University of Texas Medical School at Houston, is among these observers. A past president of the American Psychiatric Association, Ruiz calls Johnson’s work “revolutionary.” Johnson is “one of the people making the biggest contribution to the study of neuroscience and addiction.”

“Dr. Johnson is creative and innovative. His work with topiramate is the first effective [pharmaceutical] treatment of alcoholism. This is very significant. I think it is a major milestone. His topiramate research demonstrates that the problem of alcoholism is not about poverty or psychological problems or rehabilitative weakness. It is a problem in chemical imbalance,” Ruiz says.
Along with professional acclaim and global attention have come honors. Johnson has been inducted into the Texas Hall of Fame for Science, Mathematics and Technology. Johnson also has been named a fellow of the Royal College of Psychiatrists and a distinguished fellow of the American Psychiatric Association.
Addiction first intrigued Johnson 20 years ago. That fascination is unabated, but it isn’t the only subject of conversation. He’s equally curious about computer artificial intelligence and French literature. In fact, he once spoke fluent French. That’s faded, but bits remain, which tend to confound his Costa Rican wife’s efforts to teach him Spanish.
Johnson’s interests also include New York Yankee great Yogi Berra, his favorite American “philosopher.” And though Charlottesville is nice, London still feels like home to Johnson. That’s natural—he lived longer in the United Kingdom than in the United States or his native Nigeria.
When it comes to addiction, though, Johnson’s studies reflect two key themes in his life—the lure of medicine’s great unknowns and the adventure of exploration. “Science is about the thrill of the chase and the thrill of discovery. It’s a kind of a dare.”
Any medical researcher might say that. For Johnson, though, the statement is somewhat ironic because as a young man a doctor’s life had no appeal.
“I really wasn’t interested in medicine as a boy. In fact, I was far more interested in racing cars,” says Johnson. “I used to do open-wheel racing in my youth—they look like Indy cars—and actually still do select open-wheel racing.”
Besides autos, Johnson liked language and flirted with the idea of studying law. His father, a physician and Nigeria’s health minister, nixed the idea. His boy was going into medicine.
The father pulled the son out of school at 14 and hired tutors who drilled him in science. Two years later, his parents sent a reluctant Johnson to medical school in Glasgow, Scotland. To ensure he enrolled, his mother registered him.
Though his parents sent him to college, they couldn’t make him study. Johnson skipped classes, figuring he’d flunk out. He took exams and awaited his dismissal. It never came. His grades were fine. Indeed, he earned distinction in biological sciences. The tutors had done their work well, and Johnson was firmly set on the road chosen for him. He graduated from Glasgow in 1982. At age 22, he was a physician.
A specialty did not come early or easily. Johnson ultimately chose psychiatry, attracted by the mysteries of the human mind and its diseases. He became board certified, yet, he knew patients would not be his focus.
“I just wasn’t a hospital-type doctor,” he said. “I was far more interested in research than clinical practice.”
So he returned to school and eventually earned a master’s degree and two doctorates. Johnson’s studies became more focused as he advanced. However, he initially wasn’t precisely sure about his thesis topic. An Oxford professor suggested he look into an antidote for alcoholism. The idea was challenging because while the problem was big, it also was little understood.
“Our knowledge about addiction was quite poor. In fact, everything we knew—really knew—probably could be written on the back of a postage stamp,” he says.
In addition, Johnson had no firsthand experience with the condition. That, he believed, was a plus. “Many psychiatrists working with addicts have had family members or friends who were addicted. I had no personal connection with addiction. I came to the subject without preconceptions or prejudice,” he says.
Johnson also was unencumbered by myths. He didn’t accept the prevailing view, which dated to the 1930s, that addiction was a moral failing. He insists it isn’t.
“It has a biological dimension, just like high blood pressure and diabetes. Addiction is a disease of the brain,” Johnson says.
Other leading physicians share this view. It’s gained ground during the past three decades due to advances in brain imaging, data from human and animal tests, and greater understanding of genetics, and brain chemistry and functioning.
Even as our understanding of alcoholism increases, some medical professionals believe that traditional therapy holds the key.
“It is a disease of the brain, but it’s a multifaceted disease. It has a spiritual component, a behavioral component to it. Our experience tells us that having the network of support and recovery is what really makes the difference,” Dr. Kevin Clark, medical director at Hazelden, a Minneapolis treatment center, recently told CNN.
While traditional therapy is important, alcoholics like Tom agree with the new medical thinking that sees addiction as an unimaginably powerful force.
“I don’t think you can just quit,” he says. “One doctor told me: ‘Quit drinking for 30 days and you’re done.’ I don’t think that’s true.”
Tom also believes nobody starts out to become an addict. Alcoholism is a progressive disease.
“I’d been a casual drinker since I was a teenager. I wasn’t hugely interested in it. Sometimes, we’d find a way to get beer on weekends when I was in high school. But I wasn’t drinking daily once I got out on my own. I drank very little,” he says.
That changed after the football game. Tom began an evening ritual of mixing a drink as soon as he got home from work. He’d keep drinking until supper, developing a pleasant buzz. He loved summer with its long days; the evening meal came close to dark, which gave him extra time with his vodka. He started making the cocktails stronger. He bought liquor in a 1.5 liter bottle, finishing it in a week or less. A gregarious man, he looked forward to well-lubricated weekends with friends.
Tom said he never missed a day of work, although hangovers made getting out of bed harder and harder.
“I’d wake up in the morning, feeling awful, and I’d say: ‘You got to get cleaned up. You got to stop this.’ But no matter how bad I felt during the day, as it got closer to 4 or 5 o’clock, I started looking forward to a drink,” he says.
Tom began to wonder: Do I need help? That’s about the time he spotted a newspaper ad with a headline that grabbed him. It read: “Do you drink too much?”
The ad was designed to attract volunteers for one of the roughly 10 ongoing addiction trials supervised by Johnson. This one was for topiramate. Discovered in 1979, the FDA has approved the anticonvulsant for treating epilepsy and migraines. Intrigued with the drug’s functioning, Johnson theorized it might help addicts. He began researching its potential.
In 2003, he discovered that topiramate is an effective treatment for alcoholism. Testing showed that it reduced addicts’ craving for alcohol. Patients taking the drug were four times more likely to reduce heavy drinking and eight times more likely to stop drinking than those taking placebos and receiving behavioral counseling. Plus, topiramate helped lower cholesterol, body mass index, liver enzymes and blood pressure. It also reduced sleep disturbances. It also may curb the start of cirrhosis, the liver scarring that can kill heavy drinkers.
On the other hand, topiramate can produce side effects, including numbness, tingling sensations, changes in taste, weight loss and problems with thinking clearly, especially with word recall.
Over the years, hundreds of patients have participated in Johnson’s topiramate tests. In late 2008, Tom became one of them. After seeing the “Do you drink too much?” ad, he entered the trial and began a regimen of medical examinations, completing questionnaires and taking pills. Because the test continues, Tom does not know whether he received topiramate, placebos or some mix of them. However, he says his life has changed.
“About a month into the program, my craving decreased. The further I went along, the lower it went until it almost disappeared,” he says. “The cravings are less, although they sometimes flare up.”
Tom’s goal is not abstinence. He wants to drink socially and to enjoy an occasional beer. So far, he’s quit liquor and his afternoon cocktail habit.
Until the trial is complete, Tom won’t know for certain if his experience was due to topiramate. But others who did take the drug have had similar outcomes. These cases plus Johnson’s data suggest that we may have reached a major milestone in pharmacological treatment of alcoholism. Some medical experts even suggest that it may usher in a new era of addiction care, similar to what Prozac achieved for depression in the 1980s.
Ruiz believes that topiramate actually heralds something much larger. He sees Prozac as important, but it was the next logical step in the evolution of pharmaceuticals for treating mental illness. Topiramate, on the other hand, is a leap forward, changing both treatments and the way doctors view the disease.
Given what topiramate has done in opening new vistas, many people hope that an addiction cure may be on the horizon. If so, Johnson says, it’s a distant one.
“We are nowhere near curing addiction,” he says. “But I think we’ve come a long way in understanding how the brain reacts to drugs.”
The road ahead remains long due to our current knowledge—or lack of it—about the disease. Its complexity is humbling. Not only are biological issues at work, but so are psychological, cultural and social ones. These combine to affect each person differently, making a medical solution daunting.
So, a “cure” that leads an addict to abstinence is far away. However, as Tom’s situation suggests, it may be possible to end an alcoholic’s craving, to reduce his consumption to controllable levels.
“How far away is that kind of cure? Within my lifetime, I hope. Maybe as soon as 20 years,” Johnson says.
Looking far into the future, Johnson sees remarkable possibilities for addiction medicine. Ultimately, science may develop both gene and immune therapies, including vaccines. The next big step could be the creation of pharmaceuticals to address addicts’ needs based on their type and stage of addiction as well as their individual biological compositions.
Despite the challenges, Johnson is upbeat and excited about what lies ahead. That’s his nature. It’s no accident that his favorite novel is The Famished Road. Written by fellow Nigerian Ben Okri, it’s about a life of spirituality, a journey of hope and a story of adventure, adversity and triumph.
In some ways, the book seems an apt metaphor for medical research and Johnson’s approach to it—and belief in what it can achieve.
“The researcher’s work is long and painstaking, and there are lots of failures. You can’t give up too easily. It’s necessary to take the risks, to challenge ideas and follow through,” he says. “You have to be an optimist to be a scientist.”
Balancing act in the brain
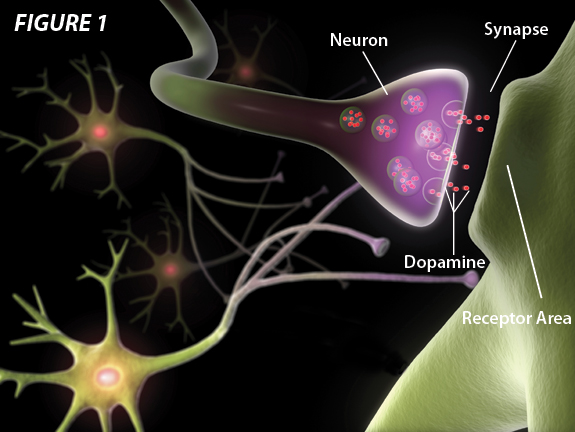
Dopamine is a brain chemical. It serves as a neurotransmitter—a messenger carrying signals between nerve cells known as neurons. These neurons communicate by sending electrical signals that are conveyed to receptors across a small gap called the synapse. Dopamine is released into the synapse, and binds to the receptors of another neuron. In order to maintain balance, some nerve cells release an inhibitory neurotransmitter (gamma-aminobutyric acid, or GABA) that works to prevent the receptor from being overstimulated.
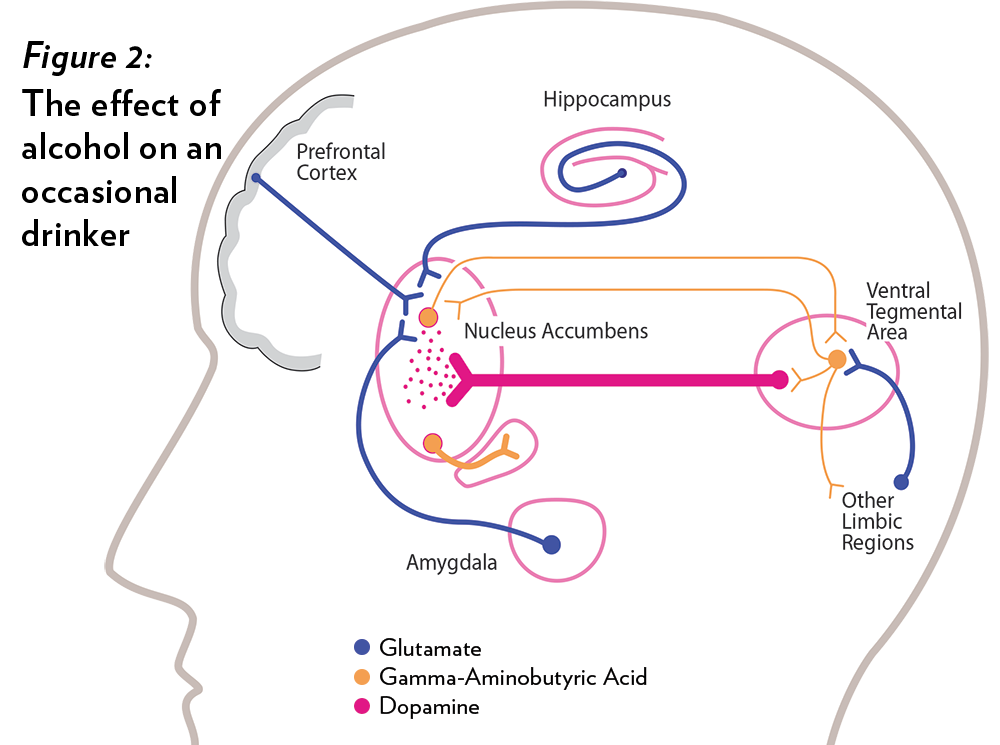
The natural release of dopamine is the key to pleasure. When we eat, drink or have sex, dopamine floods the brain’s reward system (the nucleus accumbens, ventral tegmental area, hippocampus, amygdala and other parts of the limbic region). Glutamate, another brain messenger, also comes into play by exciting dopamine neurons.
Alcohol and illicit drugs hijack the natural process by releasing huge amounts of dopamine. Resulting feelings are powerful and, ultimately, irresistible. When people try to repeat the experience, that repetition disrupts the normal balance of brain circuits. In cases of chronic abuse, or addiction, behavior can become compulsive.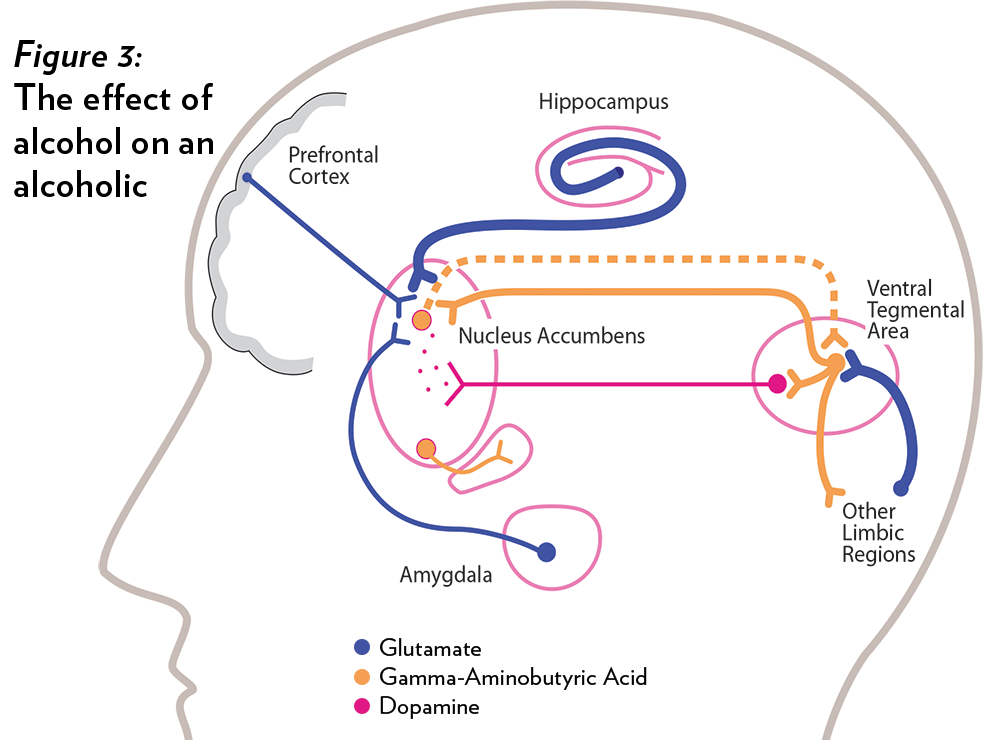
The brain adjusts to repeated surges by making less dopamine or shutting off receptors. Eventually, these reactions reduce an addict’s ability to sense pleasure. That leads to larger dosages of addictive substances—heavier drinking by an alcoholic, for example—and an inability to enjoy normal activities.
Scientists have long known about dopamine and addiction. Early attempts to affect this relationship failed. Researchers once believed that by cutting off dopamine they could end addiction. This was too crude. Remove dopamine and a patient enters a vegetative state devoid of pleasure.
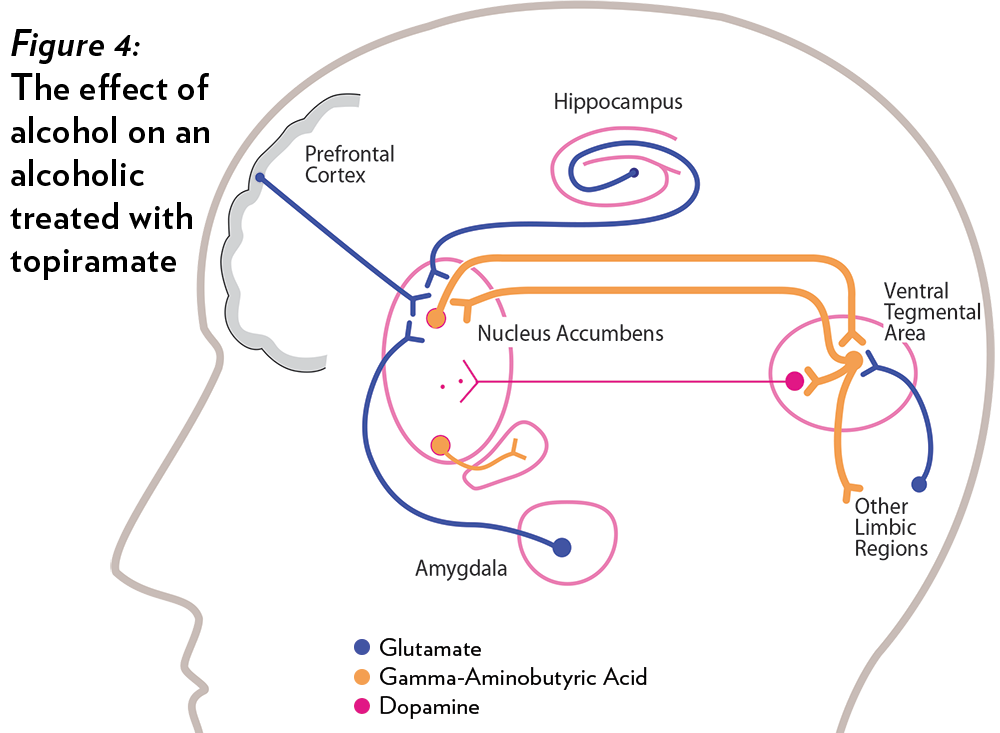
First, it promotes the action of GABA, the inhibitory neurotransmitter that serves as one of the brain’s messengers. By increasing the inhibition, dopamine’s function is decreased, and the brain does not experience the same reward. In other words, the enjoyable sensations of alcohol are reduced.
Second, topiramate inhibits the ability of glutamate—that other brain messenger—to excite dopamine nerve cells. This lessens dopamine functioning.
“The total effect therefore is for topiramate to produce a sustained suppression of dopamine in the brain and therefore a marked reduction in the pleasurable and rewarding effects of alcohol,” says Dr. Bankole Johnson, who has led clinical trials of the drug.
While this “one-two punch” is effective, it is not a cure. Instead, it modifies an addict’s desire for alcohol. This relief gives alcoholics a chance to use other treatments and therapies to regain control of their lives. Topiramate has another advantage. Addicts can take it without stopping their drinking. This is not true with many other medications.
The Food and Drug Administration has not cleared topiramate for treating addicts. Clinical tests continue. However, the drug, made by Ortho-McNeil Neurologics, can be used for seizures and migraine headaches. Johnson has served as a consultant to the firm, which provided partial funding for his research.
Help for the present, research for the future
The University’s Excelsior Program provides outpatient treatment for individuals suffering from drug and alcohol addiction.
Dr. Bankole Johnson, chairman of the Department of Psychiatry and Neurobehavioral Sciences, founded Excelsior in 2006. It offers comprehensive outpatient treatment, using pharmacological and psychological therapies.
Patients begin their treatment with a full medical examination and psychological and psychosocial evaluations. These occur in Charlottesville over a two-week period. Afterward, patients return once a week for 12 weeks or more for medication management and therapy. These are followed by monthly visits for nine months. If needed, treatment can be arranged for health problems tied to addiction.
Each patient is assigned a personal liaison who coordinates scheduling, travel and other services.
Excelsior reports a 70 to 80 percent success rate, one of the nation’s highest for outpatient clinics. This compares to a 60 to 75 percent relapse rate in the first month for inpatient rehabilitation facilities.
In 2007, Johnson also founded ADial Pharmaceuticals, a biotechnological company focused on researching and developing medications to treat addiction. Two drugs, both of which address alcohol-related disorders, are ready for phase III clinical trials. ADial, which has a partnership with the UVA Patent Foundation, is seeking to work with an established pharmaceutical company to commercialize its two lead drugs by early 2013.